


The People-Centred Framework is a country-led, data driven, process used to identify and prioritise interventions for the care and prevention of TB. The framework is used to identify, and address (through ‘interventions’), gaps in the TB prevention and care programmes, and to model the costs and benefits of the interventions. The interventions are then prioritised based on their impact and cost and, subject to available funding and prioritisation, incorporated into the National TB Strategic Plan (NSP). The implementation of the People-Centred Framework in multiple countries has shown that the process is flexible and can be adapted to meet the requirements, resources, and constraints at the individual country level.
A data driven approach
Data driven decision-making and stakeholder engagement are central to the People-Centred Framework process.
Data from National TB Programme and other sources is consolidated and analysed to create a holistic overview of the country’s TB epidemiology. Stakeholders are also actively engaged to evaluate, and identified gaps in, the existing National TB Programme, and to identified and prioritise interventions.
Crucially, the approach does not only look at data from patients who have received TB treatment, but also models the needs and perspectives of persons living with TB who:
- Do not access the health system
- Seek care but are not diagnosed or notified
- Are diagnosed as having a TB infection but are not successfully treated
Adapting the People-Centred Framework process to meet your country’s needs
The flexibility and adaptability of the People-Centred Framework has been central to the success of the approach. The key to adapting the People-Centred Framework process to meet country specific needs is to retain the core elements of:
- Utilizing data driven decision making to inform policy makers
- Engagement, and active participation, of stakeholders in the NSP development process
- Seeking out and modelling the needs and perspectives of “missing people with TB”
Country Case Study 1: Namibia Accelerating the People-Centred Framework process
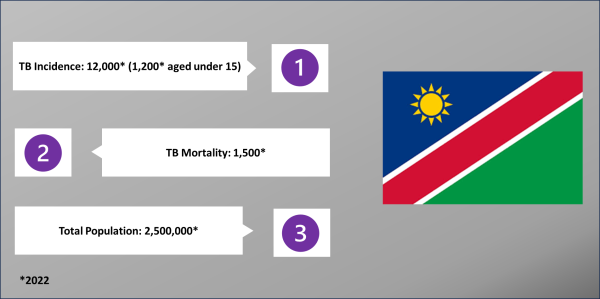
The Namibian National Tuberculosis and Leprosy Control Program (NTLCP) had just two months to develop its’ new NSP. In contrast, the traditional planning process for the development of a new NSP would normally take –six to eight months and the recommended timeline to complete the People-Centred Framework process is three and a half months.
The People-Centred Framework process had to be accelerated to accommodate Namibia’s deadline while still analysing the evidence from Namibia’s TB programme and engaging stakeholders to identify and prioritise initiatives.
Fortunately, the NTLCP had recently conducted an external program review and created a picture of the epidemiological situation of TB in Namibia. This data formed the basis for the analysis of Namibia’s national TB programme, and the identification, and prioritisation, of new interventions to prevent, and care for persons with, TB infections.
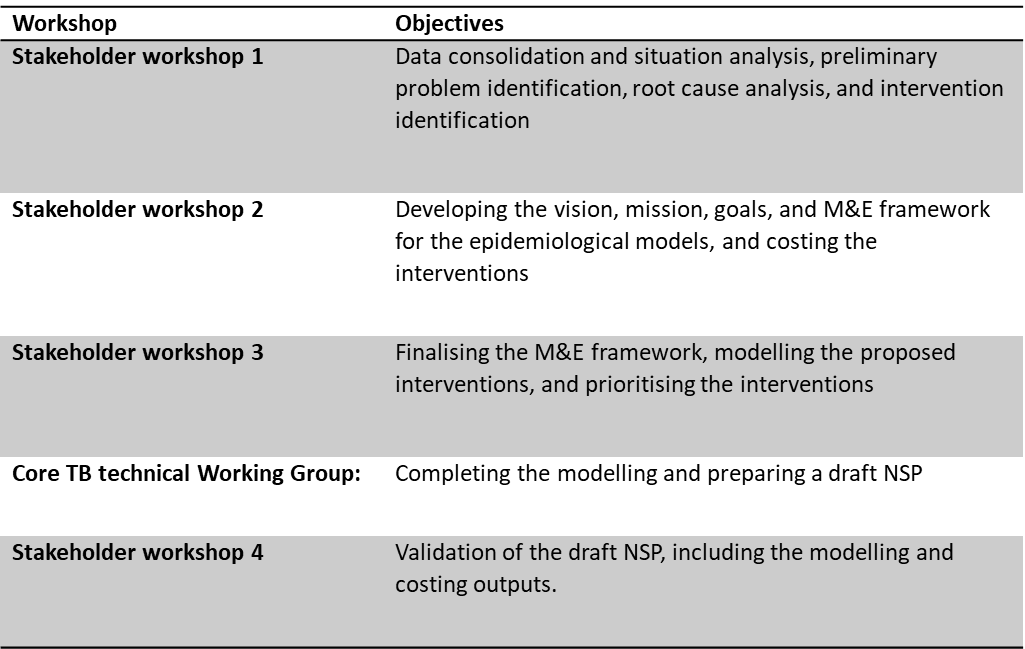
The process in Namibia included four stakeholder workshops attended by NTLCP staff, WHO consultants, regional coordinators, university staff, civil society representatives, TB and leprosy patient organizations, and KNCV TB Plus consultants. These stakeholder workshops were held in a compressed schedule with two of the workshops, five days each, held back-to-back over a period of two weeks.
Similarly, a core TB technical team was created to complete the modelling, and, under the leadership of the WHO, prepare the draft NSP. This draft NSP was then presented to the stakeholders for validation.
Utilizing the People-Centred Framework, and the WHO data, together with the support of the WHO, Namibia’s NTLCP was able to complete the new National Strategic Plan in record time and met its’ deadline.
Country Case Study 2: Nigeria Fusing the People-Centred Framework process and the traditional NSP planning process
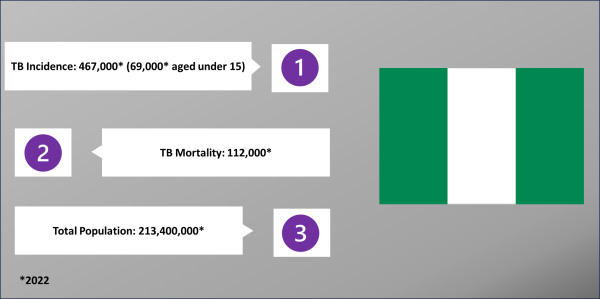
The Nigeria National Tuberculosis, Leprosy, and Buruli Ulcer Control Programme (NTBLCP) leveraged the People-Centred Framework to identify and prioritise interventions for its’ NSP and generate evidence for its’ Global Fund application.
To develop its’ new NSP, the Nigerian NTBLCP established a team to work in parallel with the traditional NSP planning team. Consisting of M&E experts and TB consultants, the team identified interventions and developed supporting evidence. The interventions and data were then fed into the findings from the NSP planning team.
The NTBLCP had completed a patient pathway analysis (PPA) in December 2022. This PPA provided detailed information on persons who may not have had access to Nigeria’s health system, or who may not have received, or successfully completed, treatment. The PPA data, together with other epidemiological and health system data from the NTBLCP was used to identify interventions for these ‘forgotten/missed’ persons.
The Nigerian team identified, and developed supporting evidence for, over 20 interventions (of which 13 were identified as high priority actions). These interventions addressed practical improvements to the network of molecular WHO recommended Rapid Diagnostics (mWRD) to support greater awareness and access for persons living with TB, improved collaboration between frontline healthcare services, and overall addressed gaps in data for people living with TB.
Country Case Study 3: Rwanda: Utilising the People-Centred Framework process to extend the NSP
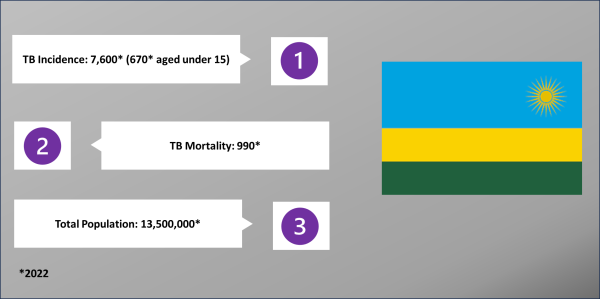
With its’ 2019 – 2024 NSP drawing to a close, rather than going back to the drawing board, Rwanda decided to extend its’ NSP until 2027. The NSP extension focused on the same priorities, but set new targets and identified new interventions to achieve the country’s TB prevention and care goals.
The People-Centred Framework team in Rwanda focused on identifying at unseen risk groups and improving Rwanda’s TB models.
The team analysed previous epidemiological reviews and National TB Programme data to understand TB case distribution and infection vectors. This analysis was used to reveal at risk groups who had not previously been identified under the NSP and to develop, and prioritise, new interventions.
The People-Centred Framework for TB programming was jointly developed by the Bill and Melinda Gates Foundation, The Royal Tropical Institute Netherlands (KIT), the World Health Organization, Linksbridge, TB Modeling and Analysis Consortium, and refined by KNCV Tuberculosis Foundation.The goal of the initiative is provide countries with the necessary tools and approaches to optimize their National Strategic Plans in line with the End TB Strategy, Sustainable Development Goals and country commitments. The goal of the initiative is provide countries with the necessary tools and approaches to optimize their National Strategic Plans in line with the End TB Strategy, Sustainable Development Goals and country commitments. The framework is a process for country-level planning with four primary planning steps centered on answering the questions in the figure below (right click the image to view a larger size in a new tab):
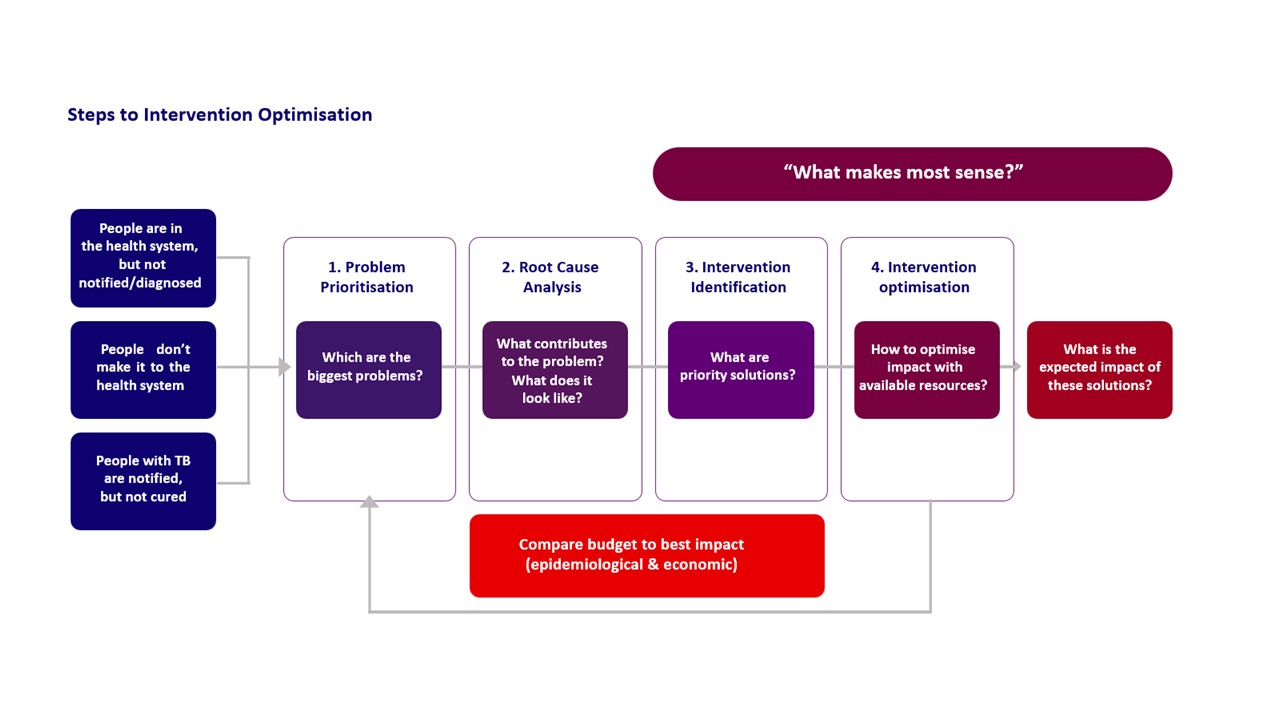 The framework is a process for country-level planning with four primary planning steps centered on answering the questions in the figure below:
The framework is a process for country-level planning with four primary planning steps centered on answering the questions in the figure below:
{kind=link}
{kind=link}